ADHD Medications: Is More Always Better?
A major new study published in The Lancet Psychiatry has provided important insights into one of the most common questions in ADHD treatment: how much medication is enough?
In their systematic review and dose–effect network meta-analysis, Nourredine and colleagues analysed data from 113 double-blind randomised controlled trials involving more than 25,000 participants with attention-deficit/hyperactivity disorder (ADHD). The study examined the relationship between medication dose, effectiveness, and tolerability across a range of stimulant and non-stimulant treatments in both children and adults.
The findings challenge the assumption that increasing medication doses will always result in better symptom control.
For children and adolescents, methylphenidate demonstrated increasing effectiveness up to approximately 45 mg daily, beyond which additional benefits appeared limited. Amphetamines showed a similar pattern, with efficacy increasing up to around 25 mg daily before reaching a plateau. Guanfacine also demonstrated a dose-related improvement, with benefits levelling off at approximately 4 mg daily.
In adults, amphetamines continued to show increasing efficacy up to around 50 mg daily, after which further dose increases provided little additional benefit. The picture for methylphenidate was less clear in adults, with some evidence suggesting continued improvement at higher doses, although the available data were less robust.
Importantly, the study did not focus solely on effectiveness. The authors also examined treatment discontinuation due to adverse effects, providing valuable information about the balance between benefits and harms. Higher doses of amphetamines were associated with increased rates of discontinuation in both children and adults. Similarly, adults receiving higher doses of methylphenidate were more likely to stop treatment because of side effects.
These findings have significant implications for clinical practice. ADHD treatment often requires careful dose titration, yet clinicians can face two opposing challenges. The first is therapeutic inertia, where medication doses are not increased despite a partial response, potentially leaving symptoms inadequately treated. The second is excessive dose escalation, where doses continue to rise despite diminishing returns and increasing adverse effects.
The study suggests that many patients may achieve optimal benefit within a relatively predictable dose range. Beyond this point, clinicians and patients should carefully consider whether further increases are likely to improve outcomes or simply increase the risk of side effects.
The findings are also relevant to shared decision-making. Patients and families frequently ask whether increasing a dose might produce better symptom control. This analysis provides evidence-based guidance that can help inform those discussions and set realistic expectations.
As with all meta-analyses, some limitations exist. Data were sparse at the highest doses for several medications, meaning estimates become less certain at the extremes of dosing. In addition, individual responses to ADHD medication can vary considerably, and treatment decisions should always be personalised.
Nevertheless, this study represents one of the most comprehensive evaluations of ADHD medication dosing to date. Its message is clear: effective treatment is not simply about finding the highest tolerated dose. Instead, the goal should be to identify the dose that delivers the greatest clinical benefit while minimising adverse effects. For many patients, more is not necessarily better.
ADHD in Children
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental condition characterised by three core symptoms: inattention, hyperactivity, and impulsivity. These symptoms can significantly affect a young person’s functioning at home, school, and in social settings.
However, ADHD rarely exists in isolation. Many children and adolescents with ADHD present with co-existing conditions, including conduct disorder, oppositional defiant disorder (ODD), anxiety disorders, and depressive disorders. Understanding this complexity is essential for accurate diagnosis and effective treatment planning.
The Importance of Effective Triage and Initial Assessment
Across many healthcare systems, waiting lists for ADHD assessments have grown significantly, sometimes extending to several years. Because of this, effective triage has become critical to ensure that young people are directed to the most appropriate clinician at the earliest opportunity.
Some services use structured screening tools such as the Development and Well-Being Assessment (DAWBA), while others have begun experimenting with artificial intelligence–assisted triage systems. These approaches can help prioritise cases and organise referrals more efficiently.
Nevertheless, a senior clinician with expertise in neurodevelopmental disorders can often be just as effective in triage decision-making. Skilled clinical judgement can help reduce duplication and ensure the correct pathway from the outset. For example, a child presenting with severe ADHD symptoms may benefit from being assessed directly by a prescriber, allowing timely initiation of stimulant medication when appropriate.
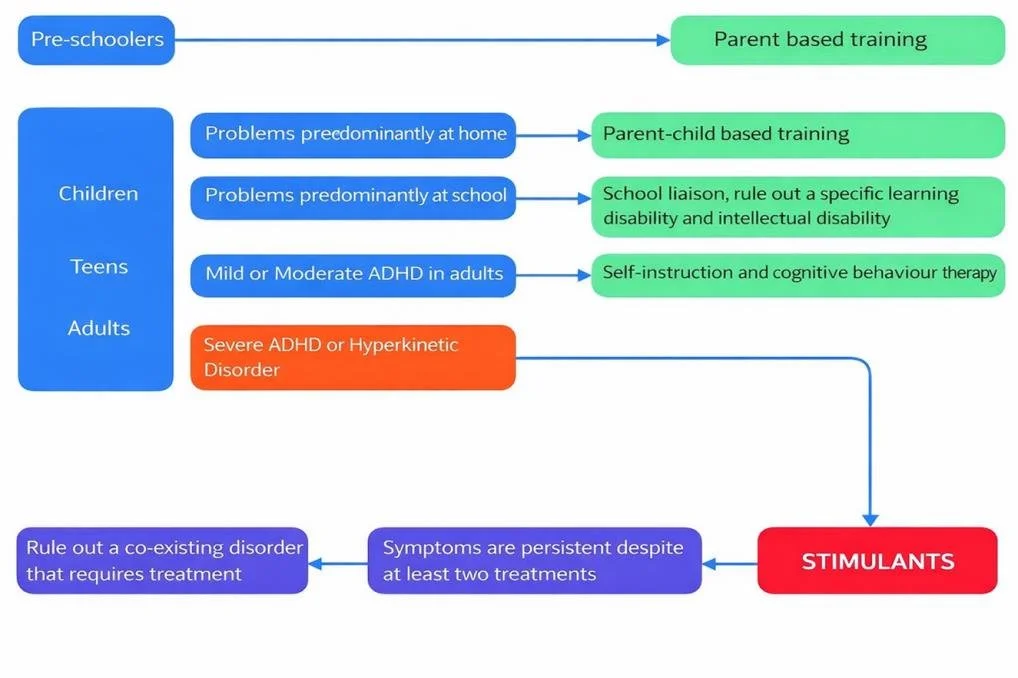
Santosh, P (2017) Stimulant medication to treat attention-deficit/hyperactivity disorder. BMJ; 358 doi: https://doi.org/10.1136/bmj.j2945
Service Configuration: Looking Beyond a Single Diagnosis
ADHD is frequently part of a broader cluster of neurodevelopmental and mental health conditions. It commonly co-occurs with:
Autism spectrum disorder (ASD)
Developmental coordination disorder (DCD)
Developmental language disorder (DLD)
Intellectual disability (ID)
Foetal alcohol spectrum disorder (FASD)
Other mental health conditions
Most individuals present with multiple, interrelated needs. However, healthcare pathways that focus narrowly on a single diagnosis risk overlooking other important conditions and support requirements.
This fragmented approach can lead to repeated and lengthy assessments, which can be both stressful for families and costly for healthcare systems such as the NHS. Integrated, multidisciplinary pathways are therefore essential to provide comprehensive and efficient care.
Treatment Approaches in ADHD
Treatment decisions in ADHD depend on symptom severity, functional impairment, and the presence of co-existing conditions.
Non-pharmacological interventions
In children and young people, non-pharmacological approaches are typically recommended as the first line of treatment. These may include:
Parent training programmes
Behavioural interventions
Psychological therapies
Educational support
These strategies aim to improve behaviour, coping strategies, and environmental support before medication is considered.
Pharmacological treatment
Medication becomes particularly important in certain situations.
Stimulant medication may be recommended when:
ADHD symptoms are severe, or
Non-pharmacological approaches have not been effective.
Importantly, stimulant medications can still be used in individuals who have ADHD alongside many co-existing conditions, including:
Anxiety disorders
Oppositional defiant disorder
Conduct disorder
Tic disorders
Autism spectrum disorder
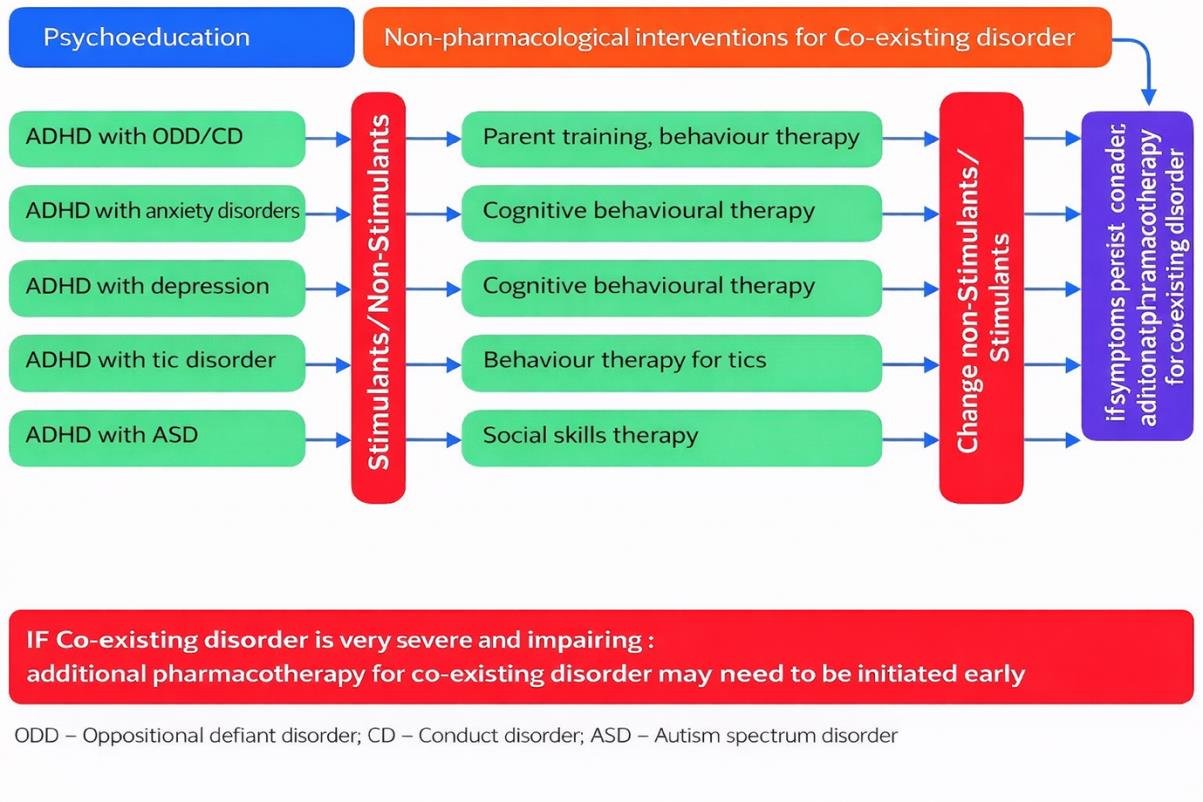
Santosh, P (2017) Stimulant medication to treat attention-deficit/hyperactivity disorder. BMJ; 358 doi: https://doi.org/10.1136/bmj.j2945
NICE Guidance on ADHD Treatment
According to the UK National Institute for Health and Care Excellence (NICE) guidelines, medication should not be used in isolation. Instead, drug treatment should form part of a comprehensive care plan that includes:
Psychological interventions
Behavioural strategies
Educational support and advice
This multimodal approach ensures that both the symptoms of ADHD and the broader developmental needs of the young person are addressed.
Looking to the Future: Monitoring and Service Transitions
As ADHD care evolves, several developments are shaping future service delivery.
Remote monitoring: When medication is prescribed, regular monitoring is required. Increasingly, this can be conducted remotely using ambulatory or personal monitoring devices, after appropriate instruction is given to parents or caregivers.
Improving transitions between services
Transitions between services — such as:
Child to adolescent services
Adolescent to adult services
Private care to NHS services
— can sometimes be complicated and disruptive.
However, with clear criteria and well-designed pathways, these transitions do not need to become bureaucratic obstacles. When services collaborate effectively, transitions can support continuity of care and prevent breakdowns in treatment.
Ultimately, the goal should always be to ensure that young people receive consistent, coordinated support throughout their developmental journey.
First published on medium: https://medium.com/p/e612e77214dc